
Clinican
Debo’rah Merritt, PhD, LPC, ABA Post-Graduate Certificate; Enid Counseling and Diagnostics Center
Background
Client was a nine-year-old male at time of evaluation; diagnosed with Autism at age three. Client had been receiving ABA therapy from this clinician for one year. Client has been diagnosed in the past with mild Mental Retardation (MR) and expressive speech delays. Additionally, he has difficulty with gross and fine motor skills. Since age five, client has received one hour of speech and one hour of OT per week at school.
Presenting Problems
- self-injurious behavior and daily aggression toward others
- tactile hyper-sensitivity; he screamed when touched
- refusal to engage others unless he knew them well; he was unresponsive to his parents’ and teacher’s attempts to discipline; reacting instead by screaming, lashing out physically at self or others
- expressive language limited to one to three word statements to communicate basic needs; not reciprocal
- play was immature and little imaginative play was present
- a one-on-one aid at school was required; in a special education classroom throughout the day
Therapeutic Goals
Increase skills in language, play and socialization, while decreasing oppositional behaviors:
- increase word statements to four to five to effectively communicate his needs without aggressive vocalizations or physical altercations 80% of the time;
- engage other children and adults with appropriate greetings with 80% success rate;
- engage in a minimum of three statement reciprocal languages with adults 80% of the time;
- engage in reciprocal play with other children for 5 minutes per free play session;
- engage in imaginative play when prompted by an adult 3 out of 4 attempts.
iLs Program Used
Sensory Motor, 60 sessions, three one-hour sessions per week, iLs Playbook (balance and visual exercises) used every session
Other Interventions Used
Applied Behavior Analysis – The Catalyst Data Collection Platform program was utilized to track behaviors. Behaviors were tracked bi-monthly over 10 trials per goal per one hour session. Behaviors were marked as independent or prompted with type of prompt used being designated. A baseline was gathered post six months of ABA treatment. These trials were completed while goal was rapport building and equipment familiarity only.
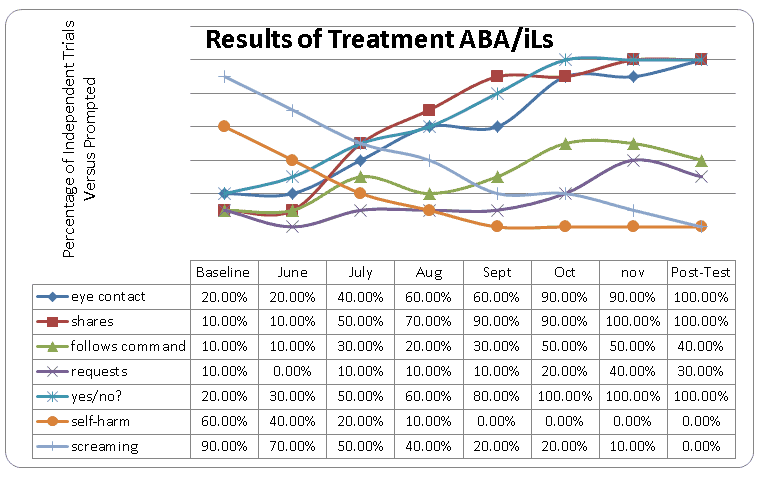
Data was then collected on each behavior every other week over 60 hours of iLs. A final data collection was completed two weeks post-treatment. Data was plotted using a graph tracking multiple data points for five different responses/behaviors utilizing discrete trial training. Two behaviors were tracked using frequency data.
Verbal, Physical, Gesture, Positional, and Demonstration prompts were utilized and documented for prompted behaviors. Independent behavior goals were then plotted on a graph as to percentage of successful trials per data tracking session. Reciprocal and Expressive Language skills were assessed including eye contact upon his name being called out, sharing of object for a minimum of one minute when asked to do so, following of direct commands by others within 30 seconds of request, use of simple statements to express needs/wants, and answering yes/no questions appropriately. Behaviors that were also tracked included screaming and self-harm.
Summary of Changes
Client was assessed one month post completion of the iLs protocol. Initial assessments were completed by his parents and teachers along with home, school and clinic observations toward completion of goals. Data was collected bi-monthly during the treatment stage using the iPad app Catalyst Data Collection Platform. The data was utilized to determine amount of progress toward goals. The final assessment utilized the Vineland Teacher Report form and the BASC-2 completed by his parents and his teachers along with a post observation utilizing data tracking.
Client’s teacher was initially upset by the ABA counseling sessions taking place three times a week in the morning resulting in the client coming to school 45 minutes late. Two weeks after initiation of the new treatment combination of iLs simultaneously with ABA therapy, the teacher stated that she wished the therapy was every day. She stated that on the days he started with ABA/iLs therapy, he was less aggressive, followed directions more, required less prompts and was on task more often.
Within the first month, client’s parents noticed a decrease in self-injurious behaviors, a decrease in screaming, improvements in sleep and more attempts at vocalizing needs.
Clinician noticed improved mood, decreased anxiety, sustained attention during sessions, improvement in gross motor skills, and decrease in aggression to self. A baseline was collected and then treatment data collection began at week two of ABA/iLs treatment, iLs session #5. Data was collected every two weeks.
Pre/Post Assessments
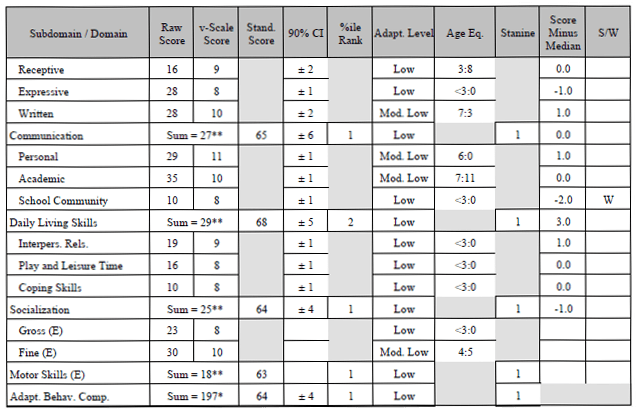
Vineland Adaptive Behavior Scale
- Pre-therapy: Low Communication (1%), Daily Living skills (2%), Socialization (1%) and Motor Skills (1%).
- Post-therapy: increase of adaptive functioning across all Composite Scales. Communication skills increased from SS 65 to 79, Daily Living Skills increased from SS 68 to 75, Socialization increased from SS 64 to 80, and Motor skills increased from SS 63 to 82.
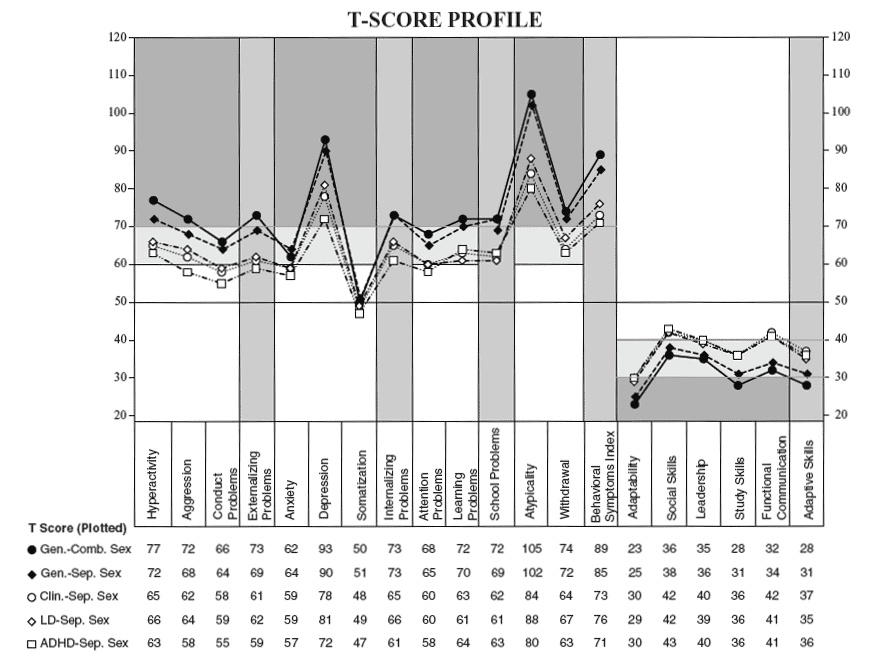
BASC-TRF pre/post assessments showed clinically significant finding in the following areas: Overall Behavior Index, Depression, Atypical, and adaptability (based on norms from a Learning Disability Separate Sex population). The BASC suggested a clinically significant decrease in Depression from clinically significant to within normal range (T-score 81 to 56) and atypicality decreasing by 18 points (T-Score of 88 to 72).
Recommendations
The combining of iLs with ABA therapy suggests an increase in skill attainment over ABA therapy alone. iLs in combination with other therapies is a powerful combination in that it works on a bottom-up principle rather than top-down. iLs utilizes specifically treated music (and specially engineered auditory equipment) to engage the brain in the process of learning while reducing sensory and mood challenges. This sensory input allows the child to be grounded, present and available for the benefits of ABA therapies. It is recommended that more studies using this treatment combination be completed using an ABAB design in order to better document the increased therapeutic benefit of the use of iLs as a tool during ABA therapy.
In addition, it is recommended that the recently developed iLs Pillow be utilized before the ABA/iLs therapy is initiated. The iLs Pillow was not available at the time of the treatment provided during this case; however, it has become a standard protocol in this clinic. The protocol involves the utilization of this device at home when the client goes to bed. The iLs Pillow delivers music through vibration and serves to help those with auditory hyper-sensitivity acclimate to auditory input prior to beginning an iLs program. A secondary benefit is that it assists clients with falling and staying asleep, which of course has cognitive, emotional and social benefits.
Comments by Ron Minson, MD, iLs Clinical Director
The impressive results from a combined approach of ABA therapy and iLs speak for themselves. One can only imagine the relief to the parents, family and teachers that his screaming went from 90% of the time to 0%!
The clinician rightly emphasizes the importance of sub-cortical processing (the “bottom-up” effect of iLs) to support learning and cognitive function. I have often emphasized the importance of establishing a good sub-cortical foundation before addressing higher learning and conscious control of behaviors. However, this case beautifully illustrates that a multi-sensory sub-cortical approach may be done simultaneously with higher order learning and behavior therapies. I can see that doing so may further accelerate the speed at which learning and behavioral control is established as these approaches work hand-in-hand to improve brain function at all levels.
An important footnote: Taking a child out of school for an effective therapy is not a threat to their learning. This case strongly points out that fact. Often a child is not benefiting from the instructions in the classroom, yet teachers fret unnecessarily over losing class time. What is the value of leaving a child in the class where they will experience more frustration, embarrassment and emotional pain because they can’t perform up to expectations?


 © 2026 Unyte Health US Inc.
© 2026 Unyte Health US Inc.