
iLs Associate:
Amy Dubey, OTR, CBIS
Organization:
Abby D Center, Petoskey, MI / Therapy Solutions, Wolverine, MI
Client:
“JN” 13-year-old male
Background:
JN was a normally functioning 3½-year-old when he was involved in an auto accident. Neuroimaging revealed hemorrhages, fractures with compression of the left ventricle. He had a craniotomy to reduce pressure and was put in an induced coma shortly after the time of injury. He was in the hospital for 2 months. He has been diagnosed with brain injury, ADHD, anxiety and has trouble sleeping.
Initial Presenting Problems:
JN required maximal verbal cues for functional task completion, his social skills were not age appropriate and his auditory self-stimulation was disruptive to those around him. Deficits in visual receptive executive functioning, fine and gross motor skills were significantly impacting daily activities, social and academic success.
Therapeutic Goals:
- Engage emotionally and socially with family and friends
- Follow simple directions for ADL’s
- Attend to tasks for 10 minutes or complete
- Cease making noises
- Increase foundational visual skills for academic, home, and community success
- Engage in simple conversation with family and friends
- Gain hand dominance
- Improve his fine motor skills for academic and ADL success and independence
iLs Program & Other Interventions Used:
JN received 26 90-minute treatment sessions, three times a week with the iLs Pro in conjunction with Occupational Therapy.
Summary of Changes:
The changes are perhaps best seen through the video in June taken on the first iLs session, and the after video taken in August on one of the last sessions. JN’s ability to complete the playbook activities and the amount of coaching necessary changed dramatically. Each video also shows his handwriting sample on that day.
Motor Free Visual Perception Test – Third Ed.
Before iLs JN required maximal verbal cues to focus and attend to the tasks. His difficulty and inability to attend did not allow him to complete all the testing. Post-iLs JN was able to complete the entire test.
|
Pre iLs Program |
Post iLs Program |
|||
| Visual Discrimination |
7 / 8 correct |
87% accuracy |
7 / 8 correct |
87% accuracy |
| Form Constancy |
3 / 5 correct |
60% accuracy |
3 / 5 correct |
60% accuracy |
| Visual Short-Term Memory |
2 / 8 correct |
25% accuracy |
4 / 8 correct |
50% accuracy |
| Visual Closure |
0 / 0 attempted |
N / A |
6 / 13 correct |
46% accuracy |
| Spatial Orientation |
0 / 0 attempted |
N / A |
3 / 6 correct |
50% accuracy |
iLs Checklist
The iLs checklist is a 4-point Likert scale style; 0 = does not apply, 1 = rarely, 2 = often, and 3 = always; lower scores are better. The scores in ( ) are post-iLs program.
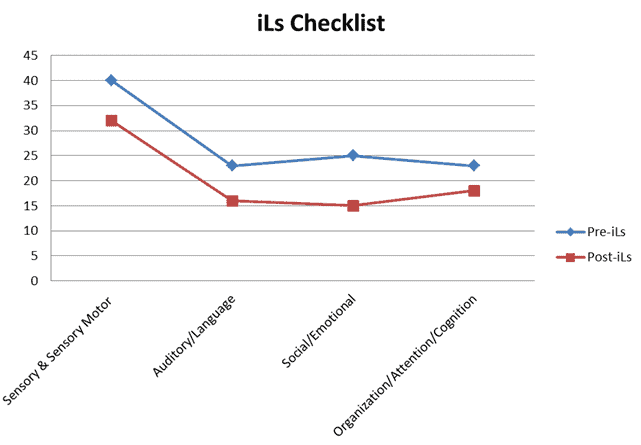
His parents reported gains in every category of the iLs Checklist.
Sensory & Sensory Motor (Pre-iL Total Points 40; Post iLs Total Points 31)
3 (2) bothered by background noise, loud, unexpected sounds
3 (2) avoids eye contact
3 (2) constantly on the move, seeks intense crashing or rough play
3 (3) has difficulty sitting still, wiggles a lot, especially if trying to pay attention
3 (3) struggles with fine motor skills, like handwriting
3 (2) cannot follow directions in a noisy environment
2 (0) bothered by textures on body, face or hands, having nails cut, hair combed
2 (0) unaware of body sensations such as hunger, hot or cold or need to use toilet
2 (3) makes disruptive noises or sounds
2 (2) difficulty learning new motor skills or those that require more than one step
2 (3) difficulty organizing personal spaces or takes a long time to perform daily life tasks
2 (2) dislikes or avoids group sports
2 (2) difficulty with visual pursuits; often loses place, eyes skip one or three lines
2 (0) has difficulty completing puzzles
2 (2) difficulty finding number or words on a page, especially during math or reading tasks
1 (2) clumsy, awkward, or accident prone, tripping or bumping into people or objects
1 (1) has difficulty identifying and distinguishing between different sounds of letters
1 (1) has difficulty judging force required for a task
1 (0) cannot find pictures hidden in background
Auditory/Language (Pre-iLs Total Points 23; Post-iLs Total Points 18)
3 (2) difficulty with spelling
3 (2) poor grammar doesn’t speak in complete sentences
3 (2) needs to be given directions repeatedly before responding
3 (1) seems to not understand what is said, i.e., poor comprehension, needs explanations
2 (2) difficulty following what others are saying
2 (2) says, “What?” or “Huh?”; needs instructions repeated, needs visual cues
2 (2) slow to react to speech
1 (2) misuses or confuses words and sounds
1 (0) is difficult to understand due to poor enunciation, can’t speak clearly
1 (1) unable to recognize or repeat rhymes or songs
1 (0) does not like to sing or hum
1 (0) difficulty interpreting tone of voice – e.g. angry vs. joking
Social/Emotional (Pre-iLs Total Points 25; Post-iLs Total Points 15)
3 (1) does not transition smoothly from one activity to another
3 (0) is not affectionate, not touching or hugging
3 (2) lack of tactfulness, acts impulsively
3 (3) response to situations appears immature for age
3 (2) anxious, bites nails, face and body are not relaxed
2 (2) easily overwhelmed, frustrated by daily life activities
2 (2) lacks confidence with new environments and new tasks
2 (0) “needy” – lacks independence, low self-reliance, low self-esteem
1 (1) irritable, short-tempered
1 (0) has difficulty making and keeping friends
1 (2) does not sleep well, can’t get enough rest
1 (0) has frequent mood fluctuations
Organization/Attention/Cognition (Pre-iLs Total Points 23; Post-iLs Total Points 18)
3 (2) is distracted easily, not able to stay on task
3 (2) has poor short-term memory
3 (3) must re-read schoolwork several times to comprehend
3 (2) has difficulty getting, finding clothes, getting dressed in the morning
3 (3) planning ahead is difficult, prefers to avoid planning at all
3 (2) disorganized with school assignments, belongings and schedule
2 (2) can’t remember sequential tasks – e.g. do A, then B, then C
3 (2) often fails to begin or to complete tasks or projects unless helped
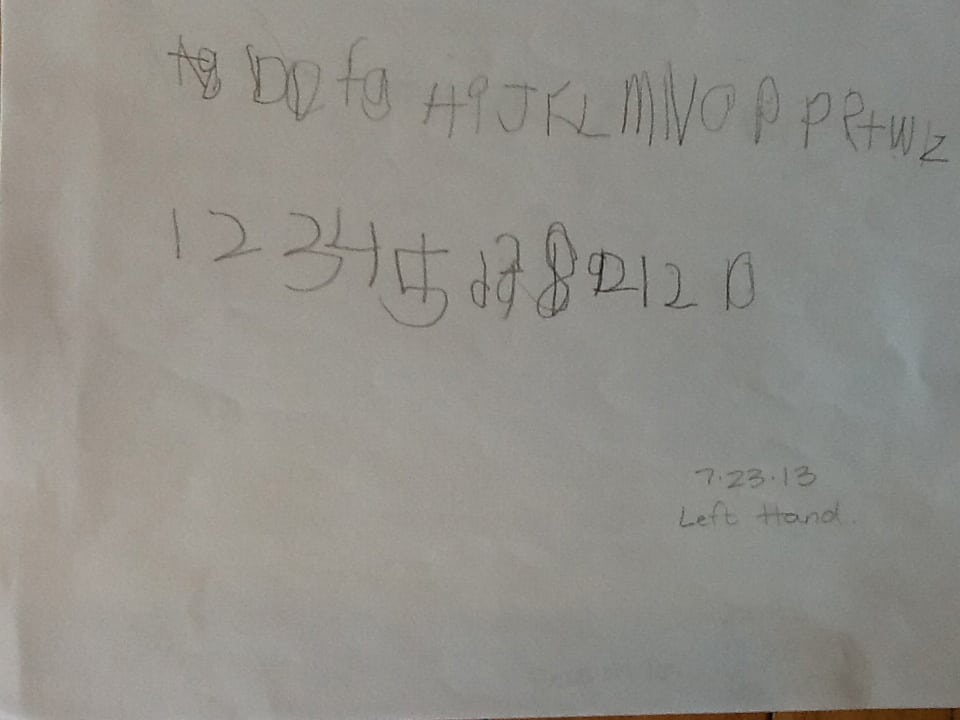
Handwriting
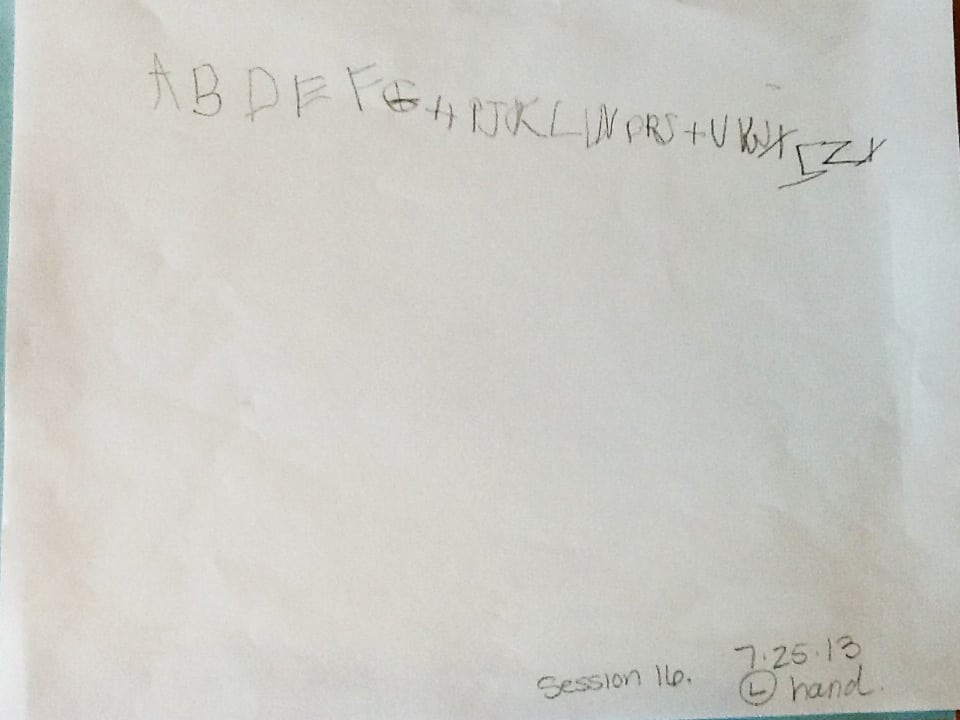
A beginning sample of handwriting was taken and maximal verbal cues were required for him to write in the correct order. He wrote large letters, made letters in reverse directions at times, and began the second line on the right side of paper and went to the left. Two samples were taken halfway through the iLs program with no verbal cues given. He fit the alphabet on one line for both samples. He missed six letters on one sample and four letters on another sample. In addition the sizes of the letters were smaller than the original sample.
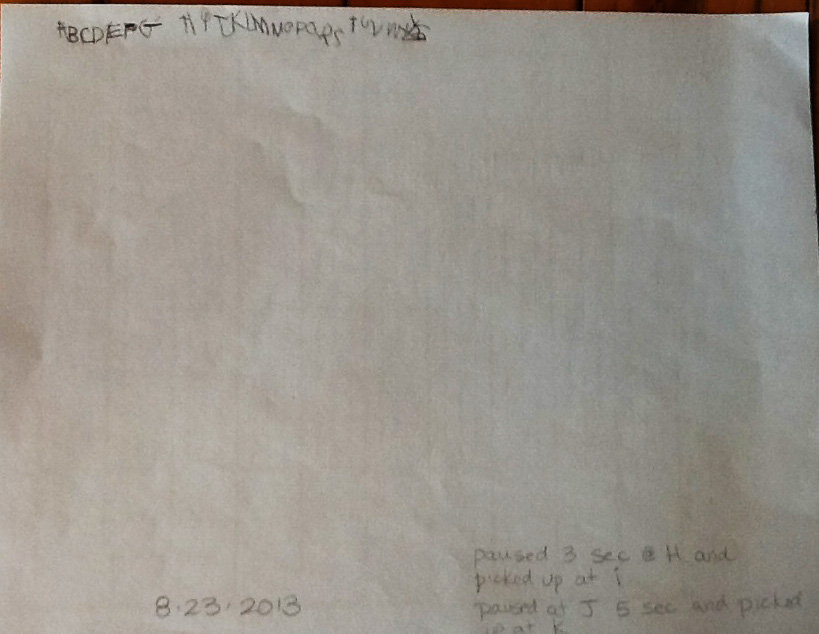
In the post-iLs program sample he demonstrated the ability to independently write the alphabet from A to Z without verbal cues. He was also able to write them in age appropriate size and on a straight line. In addition, he was distracted and paused between writing “H” and “J”, but was able to recall with accuracy where he was in the alphabet and to continue on. This is a new skill he is developing and will be of great benefit for him to increase for daily living skills, academics and social skills. (See Handwriting Samples)
Balance
Before the iLs program JN was not able to sustain balance on one foot for 20 seconds. Post-iLs program he was consistent with balancing on either leg for 20 seconds. (See Videos).
Rhythm, Timing, Coordination, Impulsivity
Pre-iLs program JN was not able to bounce a ball against the wall and catch it repetitively. Post-iLs program he demonstrated the ability to bounce a ball against the wall with one hand and catch it with the other hand repetitively with 90% success. He also demonstrated the ability to bounce a ball on the floor and let it bounce 2 times before catching it with opposite hand. This requires cognitively counting, planning motor activity, visually attending, and calculating the rhythm of the bounce for success. He was 90% successful post-iLs program.
Attention to Tasks
Pre-iLs program JN completed the dot-to-dot pages with poor visual accuracy to touch the dots and find the next letter. He required minimal assistance. Post-iLs program JN demonstrated the ability to independently find all the letters, A to Z, and to stay on the dots with each letter. At first he could only attend to the juggling of two bean bags. Now he is able to say the alphabet while juggling two bean bags. In addition, he required maximal verbal cues with most of the pre-iLs testing and only required mostly minimal cues to attend during the post-iLs testing.
Integration of Motor and Cognitive Activity
JN began the iLs program unable to successfully perform a motor and cognitive activity successfully and repetitively. By the end of the iLs program he was able to juggle two bean bags and say the alphabet at the same time with about 90% success. In addition, he was able to be interrupted by a dropped bean bag and begin (approximately) where he left.
Space Visualization
With this test two shapes were used, an egg shape and a diamond. A peg was placed in one of several available locations on one shape and presented one at a time. JN was given two shape options to choose from and place the correct shape on the sample board to fit like a puzzle. The tasks ranged from simple to complex. Pre-iLs maximal verbal cueing was required to keep him attending to the task.
|
Pre-iLs Program |
Post-iLs Program |
||
| Left Hand use |
26 |
Left Hand use |
26 |
| Right Hand use |
3 |
Right Hand use |
4 |
| Both Hands use |
1 |
Both Hand use |
0 |
| Accuracy with task |
16/30 (53%) |
Accuracy with task |
20/30 (66%) |
| Maximal verbal cues to stay on task | Minimal verbal cues to stay on task | ||
Pre-iLs program he demonstrated that maximal cueing was needed to stay on task and he has a tendency to switch hands with the task. He was slightly impulsive with the task and verbal cues had to be used to cue him to look at the items. When presented with an egg shape to match, he always chose an egg shape to trial. He was able to discriminate between the two shapes enough to select the obvious shape, but not the location of the peg in the shape.
Post-iLs program JN required minimal verbal cueing to stay on task. He improved on visual manipulation to select the correct shape to place into the puzzle piece for the peg to fit correctly. Several times he paused and thought before he selected the item to be placed.
Conclusions and Recommendations:
It is amazing to see the great improvements made in a short time, 2 months 6 days. I have worked with JN many times over the past 8 years. I have never had such good results in a short time. I would recommend further iLs programs to continue the success he has made. More focus would be on his fine motor skills, increasing duration to attention to tasks, and visual motor integration skills.
Comments by Ron Minson, MD, iLs Clinical Director:
One of the most remarkable aspects of this case is to witness how responsive the brain is to appropriate multi-sensory input in a combined therapy approach – iLs and OT. While we have seen many outstanding improvements in mild brain injury, this is a case of major brain injury where iLs was added to the therapy 10 years after the original injury. The therapist comments on his rapid improvement with the addition of iLs to his recovery from what she has experienced in the past.
The ability of the brain to improve, thanks to neuroplasticity, is truly remarkable, as demonstrated by this interesting and informative case. This helps us update our thinking and preconceptions that there is nothing more that can be done for cases with this degree of severity and long duration after injury.
“Never give up!” is a take away message from this and other cases. A remarkable rehabilitation counselor taught me that the greatest limitations to a client’s progress are the limitations we hold in our own minds as to what is possible or how much a person can accomplish.
JN Early Handwriting 7.23.2013
JN Middle Handwriting 7.25.2013
JN Last Day Handwriting 8.23.2013


 © 2026 Unyte Health US Inc.
© 2026 Unyte Health US Inc.