
Name Of Organization: Integrated Listening Australia
Associate: Joanne McIntyre, OTR, MS (Psych), PhD Candidate
Age / gender of the client: 10 year 2-month-old male
Date: Completed SSP Dec 5th-9th, 2016
Background:
Henry is a 10 year 2-month-old male diagnosed with combination ASD & ADHD. Currently taking Vyvanse 15mg for ADHD symptoms.
Henry presents with global delays in sensory regulation, sensory-motor skills and speech and language. He has an aide at school and is approx. 2-3 grade levels behind depending on the subject. He performs better with Math compared to reading and writing.
He was unable to complete Scan 3-C Auditory Processing evaluation due to inattention and difficulty understanding directions.
He had below age level visual-motor integration skills, scoring approximate age equivalence to 6 year old.
Henry tends to perseverate on objects or particular verbal dialogue that escalates when anxious.
He struggles socially and has few friends.
Presenting Problem:
- Auditory Processing
- Limited speech and language- decreased facial expression, eye contact and voice prosody.
- Delayed reading by 3 grade levels
- Decreased visual motor skills- catch a ball 3/10 trials, poor handwriting.
- Poor social skills
- Anxiety with related verbal perseveration and self-calming behaviors of finger biting and squealing.
Therapeutic Goals:
Improve attention, sensory and emotional regulation. Decrease anxiety and related perseverative speech patterns and self-calming ritualistic behaviors. Improve self-initiated interactions, eye contact and social exchange. Improve visual-motor skills to be able to consistently catch an object. Improve academics- reading, writing skills, following and completing tasks in class.
iLs Program Used:
Henry completed 25 iLs sessions from the Sensory Motor program approximately 2 weeks prior to SSP program. He had a 2 week break from iLs Listening prior to SSP.
Henry completed SSP at home with his mother. It was the end of the school year so he was picked up early each day to complete the program at home while the house was empty of other family members. SSP was completed at the same time each consecutive day in Henry’s bedroom with his mother present the entire hour.
Assessment:
Unique to this case study was the use of pre and post Quantitative Electroencephalography (QEEG) assessment. This is also known as a brain map. A brain map measures the oscillation of electrical potentials at the surface of the scalp which reflects cortical activity. The electrical activity is generated by groups of neurons firing simultaneously and measured via either individual electrodes placed on the scalp or by a cap with electrodes attached.
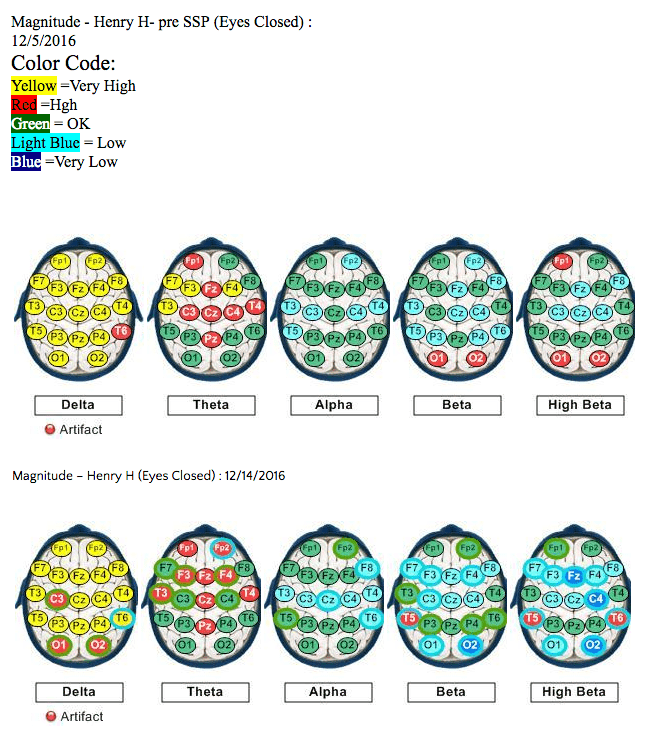
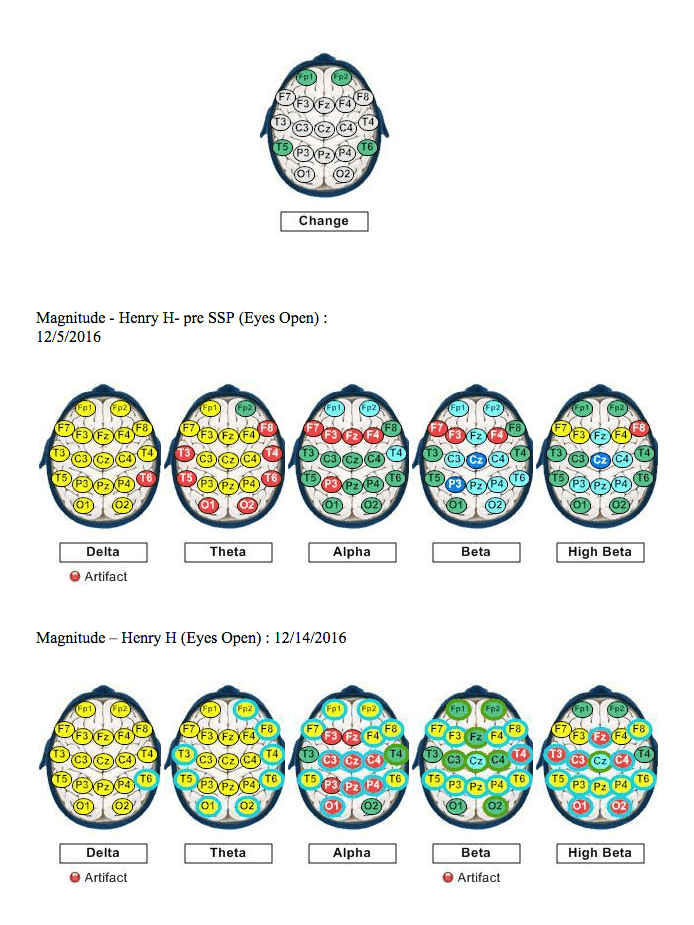
The recorded EEG is then filtered into component bandwidths, delta, theta, alpha, beta and gamma, which reflect different degrees of cortical activation. Delta waves are the slowest and of large amplitude and typically indicate states of sleep. Theta waves are also slower, larger amplitude waves and are typically more present in a brain moving toward sleep or deep relaxation. Alpha waves indicate a brain in idle mode, getting ready to either gear up for more demanding cortical task or down regulating to more relaxed states. Beta are faster, smaller amplitude waves that are present in those brain areas involved in more demanding tasks such as reading, conversing. Gamma are even faster waves and involved in more demanding task such as complex thinking, giving a speech etc.
Specific EEG patterns have been identified for different clinical presentations. For instance, ADHD typically present with too much frontal theta activity. Hence, too much slow wave activity in the frontal lobes impacts frontal lobe function. The frontal lobe is typically involved in sustained attention, impulse control, emotional regulation and executive function skills. Depression or Anxiety also have an identified EEG pattern.
In conducting an QEEG evaluation the client wears a special cap with sensors attached that record the electrical activity. The raw recording is then sent to a normative data base for processing. There are several data bases available. The maps presented below are from the New Mind Data base.
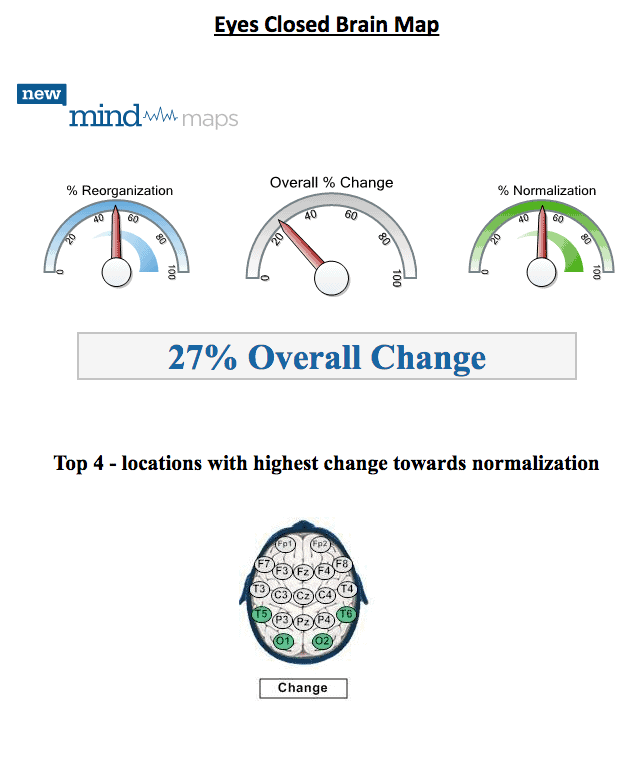
All QEEG assessments involve both an eyes closed then an eyes open recording. The eyes closed recording is considered the brain at rest, even though the brain remains very active.
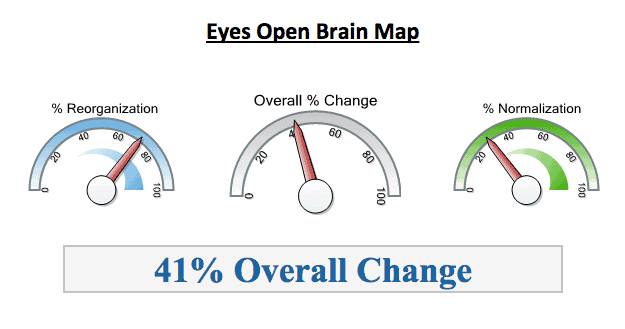
There are two sets of maps below. The first set show a comparison of Eyes open recording from prior to commencing the SSP intervention and again 2 days after program completion. The second set of maps show the same comparison but for eyes closed. The Brain Maps shown below are taken from a full report that include other measures, such as dominant frequency, connectivity, or symmetry. The EEG magnitude measure shown below reflects the average amplitude of the component bands over time.
Discussion:
The Scales at the top indicate the overall percentage of change in the EEG pre to post intervention. Any change above 20% is considered significant based on this data base. The change indicates a brain shifting, moving away from maladaptive firing patterns. It is an accepted understanding that the brain attempts to move toward optimal functioning, however sometimes the brain gets stuck in certain firing patterns and needs a nudge to find a more adaptive connection. Interventions such as iLs can often be that nudge.
When looking at the brain map showing the sites with the highest statistical percentage of change, it is interesting that occipital sites rank the highest. Often excessive fast wave activity is present for individuals with anxiety in the occipital region. Henry experienced significant anxiety and his pre-intervention brain map shows high levels of fast wave activity in the occipital region. The post map showed a shift toward more typical patterns. This would align with Porges Polyvagal Theory that the SSP helps decrease stress within the nervous system via helping the ear to attune to vocal frequencies in addition to the ability to filter background noise.
Behavioral observations reported by Henry’s mother indicated that he seemed more relaxed and was participating in social games with his sister and her friends.
Top 4 – locations with highest change towards normalization
Discussion:
The scales indicate an overall percentage of change of 41%. This indicates a brain that has made quite a shift over the course of the SSP intervention.
What is exciting to see is the top 4 locations where the EEG showed the most percentage of change; frontal and temporal sites. As mentioned previously the frontal lobes are engaged in attention, impulse control and executive function skills. The left frontal area is also engaged in positive affect, motivation and approach behaviors.
The temporal lobes are Involved in auditory processing, memory and emotional processing.
Improved processing in these areas align with Porges theory behind the SSP program.
Behavioral Observations:
No standardized behavioral measures were obtained. Mom did report the following observations:
- Less fatigue and increased interest when working on reading
- Teacher reported that Henry provided increased verbal details when called on in class
- Increased participation in social games with sibling and her friends
Observation made after completing 25 Sensory Motor sessions prior to SSP program:
- Left eye strabismus no longer present
- Appeared more confident, tried new tasks, less anxious.
Other Interventions Used:
Henry was not receiving any other clinical services at the time of the SSP program.
Conclusions And Recommendations: The SSP was successfully implemented at home.
This case study focused predominantly on pre/post SSP QEEG results. The data indicates that the SSP stimulated change in the firing patterns of the brain toward more typical patterns as compared to a normative database. The sites measuring the most change included occipital with eyes closed; frontal and temporal with eyes open readings.
Future recommendations would include completing more extensive behavioral measures to correlate to EEG data.


 © 2026 Unyte Health US Inc.
© 2026 Unyte Health US Inc.