
- Downloadable PDF
- General reference guide for using ILS with Cochlear Implants and other hearing devices
Associates Names:
Ann Brownstone, MS, OTR/L, SWC
Jennifer Aguilar, MS, CCC-SLP
Lisa Marcacci, MS, Aud.
Name of Organization:
Jean Weingarten Peninsula Oral School for the Deaf, Redwood City, CA
Abstract:
The client of focus is a five-year-old male with bilateral cochlear implants who participated in a pilot study of eight subjects at Jean Weingarten Peninsula Oral School for the Deaf. Goals included improved language skills (articulation and expression of ideas), improved auditory processing (including filtering and discrimination), gross/fine/perceptual motor skill development, and greater self-confidence. Clinical goals were not specific and were secondary to the purpose of the pilot study, which was to address the logistics of the ILS equipment with hearing devices, and to determine safety and general clinical efficacy.
A multidisciplinary team evaluated and implemented ILS for six months. After six months, gains were seen in OT, SLP and audiology. For example, results included an 80% increase in his ability to understand speech with background noise, an increase in his Test of Auditory Comprehension scores from 33% to 91%, and an increase in his Visual-Motor Integration scores from 50% to 90%. Parents, teachers and other adults all saw dramatic improvements in his self-esteem and self-expression, as he became “rather outspoken.” Similar results were seen in the other participants of the pilot study. This case study and the pilot study from which it was extracted demonstrate the potential ILS has in effecting positive changes for those who wear cochlear implants and other hearing devices.
Client: “Nathan,” five-year-old male with bilateral cochlear implants
School and Study Background:
The client of focus from an eight-subject pilot study at Jean Weingarten Peninsula Oral School for the Deaf. The purpose of the study was to investigate the effects of the ILS programs on the functioning of children with moderate to profound hearing loss or congenital hearing impairment who use hearing devices, such as cochlear implants, bone-anchored hearing aids, and hearing aids. Jean Weingarten’s curriculum teaches verbal language through intensive speech/language therapy and a classroom curriculum that supports language learning and verbal expression. There is no sign language used in this oral curriculum. There is an audiologist on staff to monitor and optimize equipment that the children have received from their primary audiologists. The students typically receive daily speech therapy for 30 minutes at the school and occupational therapy on a consult basis once per week, as needed.
Pilot Study Goals:
At the time of the pilot study, there was no information available on the use of modified music with those with significant hearing loss or impairment. Significant balance, motor, praxis, sound processing, and receptive/expressive language deficits were observable in the population at Jean Weingarten. Since these deficits are observed to improve with ILS in clients without hearing loss or impairment, the questions posed in the pilot study were related to adaptations required to deliver the sound to the children with hearing devices, and what might be the magnitude and type of improvements possible or probable in the population at Jean Weingarten.
Client History and Presenting Challenge:
Nathan was five years and five months old when he started in the study and has no significant prenatal, birth or neonatal history. Medical history includes allergies to penicillin (possibly) and several common foods. Hearing loss is bilateral and profound, diagnosed at 14 months. He received bilateral hearing aids at 18 months; subsequently, he received a left-ear cochlear implant at 22 months and a right-ear implant at 31 months.
Therapeutic Goals:
Nathan’s parents wanted to optimize his language and learning capabilities.
iLs Program Used:
Sensory Motor 1-60, then a two-week break
Reading Auditory Processing 1-40 (every other), with a one-week break after session #25
Bone Conduction: +1
Frequency of sessions: 4-5x per week, 60-minute sessions
Playbook Activities: As indicated in the Playbook
Other Interventions Used:
Other therapies during pilot: SLP (30” 5x/wk), Auditory Verbal Therapy (60” 1x/wk). It is noteworthy that parents were supported with weekly consultation to ensure the student’s engagement in the playbook activities, and for general problem-solving and question-answering.
Summary of Changes:
Pre-testing for all three disciplines (OT, SLP, audiology) took place in March, and post-testing took place in September roughly six months later.
OCCUPATIONAL THERAPY
Peabody Developmental Motor Scales, II
| Peabody Developmental Motor Scales II | Pre-ILS – March | Post-ILS – September |
| Stationary Balance | 9% | 37% |
| Locomotion | 37% | 63% |
| Object Manipulation | 16% | 37% |
| Grasping | 37% | 50% |
| Visual-Motor Integration | 50% | 95% |
Peabody Subtests: This standardized evaluation assesses a child’s motor function between the ages of 0-72 months. The test is comprised of five subtests consisting of gross motor skills and fine motor skills.
- Stationary: This 30-item subtest measures a child’s ability to sustain control of their body within its center of gravity and maintain equilibrium.
- Locomotion: This 89-item subtest measures a child’s ability to move from one place to another. The actions measured include crawling, walking, running, hopping and jumping forward.
- Object Manipulation: This 24-item subtest measures a child’s ability to manipulate balls. Examples of the actions measured include catching, throwing and kicking.
- Grasping: This 26-item subtest measures a child’s ability to use their hands. Actions measured range from the ability to hold an object with one hand to actions involving the controlled use of the fingers of both hands.
- Visual-Motor Integration: This 72-item subtest measures a child’s ability to use his or her visual perceptual skills to perform complex eye-hand coordination tasks, such as reaching and grasping for an object, building with blocks and copying designs.
Beery-Buktenica Developmental Test of Visual-Motor Integration, 6th Edition
| Beery-Buktenica Developmental Test of Visual-Motor Integration, 6th edition | Pre-ILS – March | Post-ILS – September |
| VMI – Visual Motor Integration | 86% | 94% |
| Visual Perception | 84% | 77% |
| Motor Coordination | 65% | 90% |
VMI Subtests:
- The VMI test offers a developmental sequence of geometric forms for drawing imitation or copying from a stimulus shape using paper and pencil. It is designed to assess visual and motor integration capabilities.
- The Visual Perception test offers a visual stimulus form and requires children to select a matching form from a group of choices.
- The Motor Coordination test consists of a series of forms for tracing, within a lined pathway.
SPEECH AND LANGUAGE PATHOLOGY
Testing: Selection of subtests of the following standardized tests was determined by identified areas of need, and specifically related to educational goals at the time of the pilot study.
TAC – Test of Auditory Comprehension – 5 of 8 subtests
Pre- and Post-testing: Percent Correct (PC)
| TAC – Test of Auditory Comprehension – 5 of 8 SubTests | Pre-ILS – March | Post-ILS – September |
| Recall Sequence of Three | 8/15 or 53% | 15/15 or 100% |
| Recall Four Elements | 11/15 or 73% | 15/15 or 100% |
| Recall Five Elements | 6/15 or 40% | 13/15 or 87% |
| Recall Sequence of Three in Noise | CNT | 7/9 or 78% |
| Recall Five Details in Noise | CNT | 9/10 or 90% |
CNT = could not test; beyond skill level of subject
CELF-P2: Clinical Evaluation of Language Fundamentals, Preschool, 2nd Ed. – 2 of 3 subtests
Pre- and Post-testing: Percentile Rankings (PR)
| CELF – P2: Clinical Evaluation of Language Fundamentals, Preschool, 2nd Ed. – 2 of 3 subtests | Pre-ILS – March | Post-ILS – September |
| Structured Sentences (SS) | 63% | 25% |
| Concepts and Following Directions (CFD) | 63% | 50% |
Subtests:
- Sentence Structure (SS): A sentence is spoken and four pictured choices are offered to the subject. The subject must choose the picture that best matches the verbalized sentence structure.
- Concepts and Following Directions (CFD): A direction containing one or more concepts is presented to the subject. The subject demonstrates understanding of the direction/concepts by pointing to the appropriate items pictured on each page. Concepts tested include dimension/size, inclusion/exclusion, equality, passage of time, location, sequence and conditional concepts.
Recalling Sentences Test Results
| Pre-ILS – March | Post-ILS – September | |
| Recalling Sentences Test Results | 31% | 54% |
Description: This is an informal, non-standardized test used to measure the subject’s ability to recall sentences containing a variety of grammatical structures.
Receptive (ROWPVT) and Expressive One Word Picture Vocabulary (EOWPVT)
Pre- and Post-testing: Percentile Rankings
| Receptive (ROWPVT) and Expressive One Word Picture Vocabulary (EOWPVT) | Pre-ILS – March (SS or PR) |
Post-ILS – September (SS or PR) |
| ROWPVT | 107 or 68% | 119 or 90% |
| EOWPVT | 99 or 49% | 119 or 90% |
SS: Standard Score; PR: Percentile Rank
Description: These tests are designed to assess the receptive and expressive vocabulary mastery of a subject. Four colorful picture drawings are provided as choices on the receptive test; one colorful picture drawing is provided on the expressive test.
DEAP – Diagnostic Evaluation of Articulation and Phonology Results
| Pre-ILS – March | Post-ILS – September | |
| DEAP – Diagnostic Evaluation of Articulation and Phonology Results: | 9% | 37% |
Description:
This measure evaluates a child’s speech as it relates to articulation and/or phonological process delays and disorders.
AUDIOLOGY
Nathan was able to wear the ILS headphones over his cochlear implant processors. The optimal volume level for ILS listening sessions was determined by the audiologist.
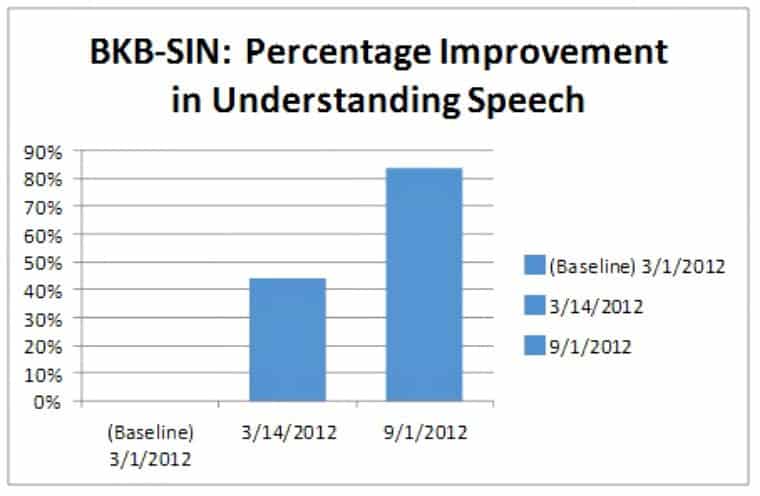
BKB-SIN (Speech in Noise) Test
Nathan obtained a score of 8.5 dB at his pre-test on the BKB-SIN test. One week later, the BKB-SIN test was accidentally re-administered. It was very surprising that his score had already improved by 2 dB. His mother reported that he had listened to the ILS program for just one week, or four to five sessions (one hour each session). Nathan returned for post-testing after five months and demonstrated an additional 2 dB improvement.
Description:
This test was selected to further investigate possible binaural processing improvements with ILS. In a previous study (Harper and Weiner, 2009), electrophysiological changes (increase) in the binaural summation of brainstem responses were noted pre- to post-ILS treatment, indicating an increase in communication between the two ears. For those with normal hearing, the use of two ears is necessary to pull the speech sounds from background noise. The BKB-SIN test is a group of simple sentences presented in increasing levels of background noise. The scores on this test reflect the lowest signal-to-noise (SN) ratio for comprehension of the stimulus signal (speech), at 50% accuracy. Lower numbers reflect higher skill levels. For example, an SN ratio of 5 dB indicates that a person is able to understand 50% of what is being said when the signal is 5 dB louder than the background noise. A SN ratio of 0 dB means that background noise and speech are the same volume.
DISCUSSION:
Occupational Therapist: Nathan’s percentile rankings improved by a factor of four in stationary balance, a factor of two in object manipulation (ball and target skills), nearly a factor of two in locomotion skills and visual motor integration, and significantly in grasping skills. These scores are derived from standardized measurements, so they account for aging, and the improvements are beyond what would be expected after a period of six months. On the VMI, his fine motor skills improved the most significantly. However, he did receive a lower score on the visual perceptual subtest at post-testing. Functionally, on observation, Nathan demonstrated greater self-confidence when performing motor skills, with higher levels of speed and strength when executing movements and moving through space generally. He appeared to be more “comfortable in his skin,” and he expressed his increased levels of energy through his movements, just as he expressed his increased mental energy through improved and increased expressive language, asking questions of his caregivers, and improved academic performance.
Speech-Language Pathologist: Nathan’s performance grew significantly across all areas tested. His ability to blend sounds presented verbally became quite fluent and age-appropriate. Significant improvements in speech articulation as measured by the DEAP were also seen. Phonological awareness gains may have contributed to his ability to self-monitor his own speech. On the auditory-specific evaluation, the TAC, Nathan passed subtests that were failed in the pre-test (ILS) condition. Additionally, he expanded his ability to listen in noise, a task he was unable to attempt in the pre-test (ILS) situation. His progress reflects an increase in skills for auditory memory, auditory sequencing, auditory comprehension, and auditory figure-ground.
Language-specific testing using the CELF-P2 revealed significant gains in Nathan’s ability to follow verbal directions. He appeared to have an increased auditory memory for longer units of information and concepts (spatial, temporal, conditional and quantity) presented in sequence. This strengthened skill contributed to his increased speed and accuracy for processing spoken language. Most remarkable were Nathan’s scores on the Receptive and Expressive One Word Picture Vocabulary Tests. His growth and retention for words outpaced his learning rate prior to this study.
Audiology:
Overall improvement of 4 dB was obtained, which is very significant; studies show that improvement of even 1 dB in an SN ratio may improve understanding of speech by 20%. Therefore, changes of 4 dB in SN ratio may suggest the student who is deaf or hard of hearing may better understand what is being said in the classroom by 80%. On average it is estimated that the SN ratio in a typical classroom is +6 dB (the teacher’s voice is ~6 dB louder than the background noise). Children with hearing loss typically have up to a 10 dB SN ratio disadvantage as compared to their hearing peers. Most of these children need more than a teacher speaking louder (6 dB). They use FM systems to add volume to the teacher’s voice in order to overcome the noise of the classroom and distance from the teacher. In a fast-paced and dynamic classroom, where FM use and noise are highly variable, improved listening in noise skills supports achievement of greater independence and possibly academic success.
Teacher: Teacher observations were recorded for approximately 18 days. The following challenging behaviors were noted and recorded by Nathan’s teacher:
Several instances of silly behaviors and a low tolerance for frustrating circumstances (e.g., not being called on in class, not getting his way) were noted throughout the recording period. He also showed some urgency and impatience in wanting to communicate his ideas by repeating himself and attempting to gain attention from others. He soiled his pants three times one week and a month later had two more accidents in one week, after being completely toilet trained for years. Nathan’s teacher also reported that he seemed more alert and engaged in class, and she was impressed with observable improvement in verbal expression and initiation in the classroom.
Parent: In the first few weeks of listening, according to his mother, Nathan showed a huge increase in his physical activity level. Within this same time period, she also reported that he ate a “huge” meal of tri-tip and fries, not typical for him. Additional remarks include a robust increase in expressive language, as he spoke more confidently in public to unfamiliar adults and children. Previously, she felt compelled to stay close to him and translate or support his verbal communication at all times; after starting ILS, Nathan interacted with a face painter at a park in a confident and articulate manner, describing what his younger sister wanted. Nathan was also observed by his private auditory-verbal therapist to be much more confident and expressive in his language. His mother watched him strike up conversations with waiting room peers and their parents while he waited for his therapy, which he did not do prior to listening to the ILS programs. Along with this increase in self-expression, Nathan also demonstrated more self-confidence generally and “stood up for himself” more. His mother reported he previously was on the “soft side” in terms of temperament, but during the ILS program he became rather outspoken. He began to ask “why” questions more, so much so that his mother felt the need to implement a system where he would write down his questions in order for her to answer them later. He also asked these “why” questions regarding his parents’ directives, with a stronger sense of self and a flavor of either a (missed) three-year-old ego formation phase or very early adolescence. Nathan’s sentence structure improved, and he used more elaborate language with greater nuance. For example, his mother reported phrases like “a flower is something that is pretty and, when you give it to someone else, it cheers them up” and “almost, not quite.” His mother reported that during ILS listening, he demonstrated improved memory for new academic learning and after the pilot study, he was ahead in his curriculum at school. During the listening program, new behaviors included singing along to music on the radio, and memorization and verbal expression of text he heard previously on a CD. Nathan’s piano teacher reported his discrimination of pitches to be higher than typically hearing children, and that he was progressing more quickly in learning how to play the piano during the pilot study than typically hearing children.
Conclusions and Recommendations:
Nathan was part of a pilot study involving eight students at a school for children with hearing loss or impairment. Nathan has bilateral cochlear implants (CIs), and other subjects have bilateral devices or a combination of CIs, bone-anchored hearing aids (BAHAs) or hearing aids. Nathan was comfortable with the ILS headphones placed directly over his CI receivers (powered on), and the ILS amplifier volume level was determined by the audiologist who worked on the pilot study. The children with BAHAs and hearing aids, however, received the ILS programming from the headphones in place (headphone cups over the ears) with their devices removed, as there was significant feedback from the device when it was turned on and in close proximity to the headphones. Again, volume levels for the ILS amplifier were determined by the audiologist and were based on the level of hearing loss.
Nathan, our case study with bilateral CIs, demonstrated significant improvement in almost all areas tested, and in many functional domains as well. He seemed to “blossom” in many areas during the six months of ILS listening. Other children in the study demonstrated similar gains to Nathan’s. The pilot study had limitations in terms of sample size, lack of controls across professions and test choices and procedures; it nevertheless provides an initial template for further research. It also provides a message of hope that the motor and language development of children with hearing impairment or loss may be supported and facilitated by using ILS.

Discover the Integrated Listening System
The Integrated Listening System consists of programs that provide simultaneous multisensory input to help develop new, and reinforce existing, neural pathways governing organization of the body and brain function.


 © 2026 Unyte Health US Inc.
© 2026 Unyte Health US Inc.