
Clinician
Sandra Giglio, Professionally Certified Educational Therapist, Charlotte Christian School
Background
Client name: “M”
Gender/Age: female/12 years of age
Diagnoses: reading disorder; disorder of written expression
Previous therapies: M has received educational therapy for 2 years.
iLs was done as a supplement to her educational therapy during the last year of her therapy.
Presenting Problems
Reading disorder and written expression disorder
Therapeutic Goals
To increase fluency in reading, writing and math
To increase written expression skills
iLs Program Used
Program name: Concentration & Attention
Frequency: forty 45-minute sessions at a frequency of two-three per week over a period of five months
History
M was first diagnosed with a learning disorder in the fall of 2008. At that time she was given a full battery of psychoeducational testing.
When M changed schools in 2010 she was experiencing some anxiety in the classroom. She displayed difficulty with reading and written expression, particularly with phonetic decoding, spelling and organizing her thoughts to transfer to writing.
M’s reading fluency was extremely halted. She would use stalling techniques to help camouflage the breaks and allow more “thinking time” for decoding. She displayed multiple hesitations, repetitions and would frequently omit endings and punctuation.
M appeared to have no defined dominance. She would switch from her right hand to her left, depending on the task and the speed in which she wanted to perform the task.
M was highly distractible. She would often interrupt her thoughts and side-track with a story of something totally unrelated. Noises or activity around her would disrupt her concentration and attention.
M is a vivacious and outspoken young lady. She is a twin who plays the role of the underdog. Her twin is a high achiever and easily earns good grades. M, on the other hand, worked hard to earn the grades that she got and seemed to be in constant competition with her sister.
M’s performance in the classroom and in therapy was often sabotaged by her lack of emotional control. She would shut down emotionally if a task was too challenging or not enjoyable enough. M also had a difficult time handling failure and criticism.
Other Interventions Used
M participated in the NILD (National Institute for Learning Differences) educational therapy program offered at her school. I have been M’s therapist since 2010, and I have had a long standing working relationship with her prior to beginning iLs.
Education therapy targeted:
- Math
- Reading fluency
- Spelling
- Language processing
In the first year of therapy there was a significant decline noted in the area of written expression. M seemed to develop an aversion to writing and was quite resistant to writing activities in therapy.
M began her second year of therapy at the beginning of the 2011-2012 school year, upon entering the 6th grade. We started the year implementing the iLs Concentration & Attention Program. Sessions were limited to 45 min. to fit into the school schedule.
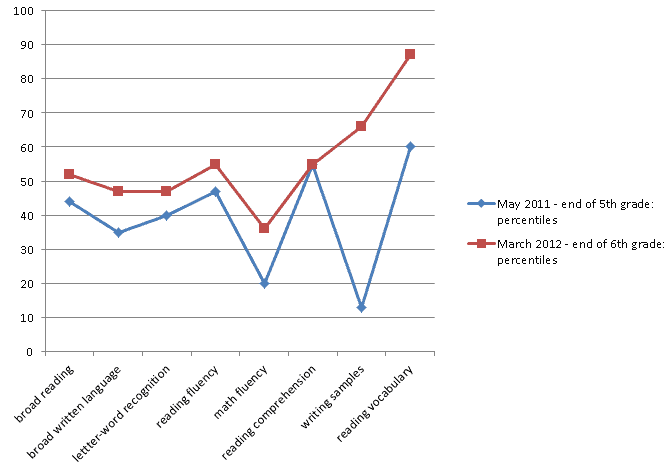
Summary of Changes (Tests, Observations, Feedback, etc.)
Results from the pre- and post-testing of the Woodcock-Johnson III Achievement Test:
Conclusions and Recommendations
Adding iLs to M’s educational therapy regime during an academic year appears to have helped her make significant gains in reading and writing. Her scores on the Woodcock-Johnson writing tests went from a percentile ranking of 13% to 66%. Her aversion to writing has decreased while her ability to write a concise and informative paragraph has increased considerably.
M also made gains in the following academic areas:
- reading and math fluency have increased
- no longer employs her stalling technique as she reads
- 13 point increase in her measured vocabulary scores
- although she continues to struggle with decoding, reading for pleasure has become her favorite pastime
- organized a reading club with her peers and is tackling more difficult books
In the areas of cognitive and emotional function:
- is much improved in her ability to handle stress
- has more control over her emotions
- has more staying power – even when not enjoying a task she will push through to completion
- is now able to show response inhibition, task initiation, planning and prioritizing along with improvements in time management
- has established dominance on her right side
As shown with the percentile data above, some of the gains were not as significant compared to the observed changes in behavior and performance. Quite often, emerging qualitative changes are not always immediately reflected in the test scores. It is also worth noting that a child with learning disabilities has often fallen behind their peers; therefore, gains made may indicate significant growth for that individual even though they are still not testing at grade level.
Prior to adding iLs to her educational therapy, M had been on a downward trend. Her academic scores were showing an overall decline each year. It seems apparent that with the addition of iLs, we have reversed this downward trend.
In light of the overall growth from this past year, I would conclude that including iLs with her educational therapy was efficacious and I would recommend that M continue with iLs therapy. The next logical step might be the iLs Reading & Auditory Processing Program, given her continuing struggle with decoding and reading fluency.
Comments by Ron Minson, MD, iLs Clinical Director
The presenter wisely remarks that qualitative changes often precede test score improvement. I would add that this is true of grades, as well. In working with children academically behind in school, I always counseled parents to not expect the grades to go up for at least a year. What we are doing in iLs is putting in place the neurological foundation for learning, improving the subcortical processing of sensory input and increasing the speed of processing. This takes time.
Once this foundation is established, learning is poised to take off. Parents need this admonition because they tend to react to their anxiety around their child’s failure by putting undue pressures on themselves, the child, the teacher and often the therapist or educational specialist, as well. This only makes matters worse and continued failure is the result. In this presentation, the child losing ground while in good educational therapy must be a fearful experience for the parents and confusing to the specialist. Until subcortical organization is established, often cognitive-based therapies and learning tools fail to reach their expected results.
I want to emphasize one of the most important outcomes, namely M having established right dominance! This is critical to improved brain organization. I would hazard an educated guess that the lack of laterality played a major role in M’s struggles. I would strongly urge that the iLs Interactive Language Program (ILP) be included in her next phase. M may very well still have a left dominant ear and will benefit from encouraging a right ear dominance which is possible with the ILP. Her difficulties continue to be with decoding and reading for which the ILP is ideally suited.


 © 2026 Unyte Health US Inc.
© 2026 Unyte Health US Inc.